ACVR Guidelines to Maintaining Residency Standards during COVID-19 (March 19, 2020)
Veterinary institutions are facing daunting challenges during these initial weeks of the COVID-19 pandemic. Among these challenges is the balance between our commitment to resident training and the reality of decreased institutional clinical caseload, adapting to infection control strategies, reduced staffing and overall personal and economic anxiety.
The ACVR Executive Council, Residency Standards Essentials Committees and Examination Directors want to support and guide Residency Directors in the coming weeks and months. We feel that the current Residency Standards Essentials will be difficult, if not impossible, for many programs to maintain.
We are suggesting the following guidelines to provide additional flexibility to the current Residency Standards Essentials.
These guidelines are outlined for the period between April 6 – July 3, 2020 (3 months). This is primarily to ensure that final year residents receive adequate “end of program” training to allow certification. This can also serve as a test period for these more flexible guidelines.
The ACVR recognizes that this pandemic will likely continue to have effects for the weeks and months thereafter. These guidelines will be reviewed and adapted as the situation evolves. It will be important for us to receive feedback from Residency Directors and residents in order to best adapt to the evolving situation.
These guidelines aim to ensure a continuity of training both for:
- Residents on clinical duty in veterinary hospitals that are on emergency only and/or are facing a decrease in institutional clinical caseload.
- Residents who are unable to be physically present for their usual clinical duty due to preventive quarantine measures or even illness.
1) Diagnostic Imaging and Equine Diagnostic Imaging
The ACVR recognizes that there exists a wealth of clinical imaging material that can effectively be used for image interpretation training, be it within individual teaching institutions or within the greater radiology community.
Clinical Training (“On Clinics”)
Most hospital caseloads have faced a serious decrease over the past few weeks. It is assumed that many are no longer able to guarantee the number of clinical cases specified within the Residency Standards Essentials.
Residents who have fulfilled their 30 months of clinical duty are exempt from the following guidelines.
To review, the DI and EDI Residency Standards Essentials require that a resident see a minimum of 4000 radiographic, 1000 ultrasound examinations, 300 CT and 200 MRI studies and spend 30 months on clinical duty.
Over the next 3-month period, this translates to clinical exposure of a minimum number of cases per resident of :
- DI and EDI 400 radiographic examinations (6 cases/day; 30 cases/week)
- DI and EDI 100 ultrasound examinations (1-2 cases/day)
- DI 30 CT examinations (3 cases/week); EDI 15 CT examinations (1-2 cases/week)
- DI 20 MRI examinations (2 cases/week); EDI 15 MRI examinations (1-2 cases/week)
- EDI 15 Nuclear Medicine examinations (1-2 cases/week)
In many programs, residents were exposed to a far greater number of cases. It is possible that a few programs will maintain these minimum case numbers even with a reduced caseload.
For the programs that cannot maintain minimum clinical case numbers, we are extending the following flexibility :
1) The definition of a clinical case is broadened to include:
- Institutional teaching case files
- Clinical cases from prior dates within the hospital PACS (i.e. use cases from a previous date, i.e. March 28, 2010)
- Teleradiology cases
- ACVR Shared KCC database cases https://acvr.org/dashboard/resources/shared-kcc-database-2/ (Keep in mind, this resource is a diplomate-only resource; the database is intended to be reviewed between mentor and mentee; not residents alone).
- Cases sourced from other veterinary radiology websites, etc…
In other words, we encourage residency programs to source cases from pre-existing digitally available case material, to compensate for a decrease in institutional clinical case numbers below the current minimum requirements.
2) Interpretation of recorded ultrasound images (still and video) is considered an adequate replacement for live performance of ultrasound examinations.
3) The same case may be reported upon by more than one resident, as long as each resident generates their own report, independent of input from fellow residents.
4) Residency programs may obtain cases from other institutions, whether they have residency programs or not.
5) The number of cases for this 3-month period may be prorated to the time the resident was scheduled to be on clinics. In other words, if a resident was scheduled to have 2 weeks of off clinics time in the next 3 months, case numbers may be reduced by the number that would be seen in a 2-week time period.
It is still expected that residents generate independent reports that will receive feedback. We understand that in many cases feedback can no longer be given in the traditional format of sit down, in-person rounds. For this reason, we are extending the following flexibility:
- Virtual live rounds. These may also be recorded to be watched by absent residents at a later date.
- Written commentary.
- The radiologist providing feedback (rounds or written) does not need to be on clinical duty. Feedback may be provided by an offsite radiologist. Where there are staff shortages, cooperation between institutions is encouraged.
Residency programs are encouraged to suggest additional (creative!) solutions to provide alternative clinical case material and feedback. The ACVR encourages a community discussion on Discourse. We also encourage that radiologists and programs with additional resources offer those resources (time, cases, feedback) to programs that may have a greater need.
Supplemental Training
It is highly encouraged that Known Case Conference and Journal/Book Club continue, using a virtual format. Should an institution be unable to provide these activities due to staff shortages, cooperation between programs is encouraged. These activities may also continue with the help of offsite radiologists.
We also encourage residents to engage in self-learning and cooperative learning. There are myriad resources available, including of Case-of-the-Month material on the ACVR website, veterinaryradiology.net, etc… The ACVR Learning Website Page is a good starting point: https://acvr.org/dashboard/resources/other-learning-websites/.
Documentation of Training
Because residency programs may not be able to maintain the minimum case numbers specified in the Residency Standards Essentials, residents are requested to maintain a case log during the next 3 months. The ACVR may request case logs to compile data around these novel training approaches, or in the case of a disagreement between a program and resident.
The case log should be as an Excel spreadsheet and include the following information:
- Name and training year of the resident
- Case details: ID or report number, name, date of examination, date of report, modality, region.
- Name of the radiologist providing feedback
Recording of supplemental learning activities is also encouraged: title, date
A template of the case log is available
It is recommended that Residency Directors (or their proxy) also establish a written plan/schedule that details where alternative clinical case material will be sourced and methods that will be used to provide resident feedback. For this 3-month period, the plan does not need to be submitted to RSEC; however, please expect that the ACVR may need to verify this plan at a later date.
Off Clinics Time
The above clinical case reporting requirements are intended to provide sufficient flexibility to accommodate off-clinics time that was already scheduled for residents for research, study, course preparation, etc.
Examples
Institution X is on emergency duty only with a 60% decrease in normal clinical activity and a radiologist on 14-day preventive self-isolation. More than 1 resident may now report on the same case, which allows maintenance of 80% of clinical case reporting for the residents. These cases are reviewed in rounds by the remaining onsite radiologist. The remaining 20% of cases are provided online from the offsite radiologist’s teaching file. Residents draft virtual reports, which are reviewed by the offsite radiologist.
Resident Y is on preventive self-isolation and does not have enough vacation/sick/off clinics time to cover this time period. This resident may double up reporting on active clinical cases offsite and attend daily rounds virtually. Alternatively, he/she may create virtual reports on assigned cases from an offsite collaborating radiologist’s teaching file (or another source). These reports are reviewed by the offsite collaborating radiologist.
2) Radiation Oncology
Clinical Training (“On Clinics”)
For residents who have completed the requirement for a minimum of 18 months of radiation oncology training before March 13, 2020:
- No further documentation to RO-RSEC is required. These residents are encouraged to remain in contact with their RO program directors to devise a weekly plan for self-study or/and clinically-related duties (such as remote consulting or remote treatment planning).
For residents who have NOT completed the requirement for a minimum of 18 months of radiation oncology training before March 13, 2020
- Residents must work with their program director to devise a written weekly work plan starting the week of April 6, 2020 (this can be a short as 1-2 daily bullets or a paragraph), which must be signed by the resident and the residency director. For each week that the resident’s normal caseload is limited by hospital closures or personnel limitations, documentation should be provided.
- If these weeks number beyond 12 weeks (3 months) of the program, additional, supervised clinic training may be required. In these cases, the RO-RSEC will work with the residency mentor and candidate to define how a trainee receives credit for additional supervised clinical training, as it may have to occur following the completion of a trainee’s current residency program for residents due to complete residencies in July 2020.
3) Examinations
Preliminary Examination DI
As of this writing, it is expected that the DI preliminary examination will take place on the scheduled date in August 2020. Provisions are being made that the exam may take place virtually using Exam Soft, without the need for travel and that videoproctoring will be used.
Certifying Examination RO
As of this writing, efforts are underway that the RO certifying examination will take place on the scheduled date in August 2020. The feasibility is being investigated of holding the exam virtually with videoproctoring using Exam Soft, without the need for travel.
Certifying Examination DI and EDI
As of this writing, plans have been maintained to hold the examination on the scheduled date in August 2020, at the Oquendo Center in Las Vegas, NV, with an additional examination in December 2020. Because it is likely that travel restrictions will still be in place for at least some candidates, the possibility of holding the exam remotely at various institutions is also being assessed. The possibility of deferring the examination until December 2020/March 2021 is also being assessed. It is the ACVR’s wish to prevent a significant delay in certification, knowing the potential impact on candidates’ entry into the profession.
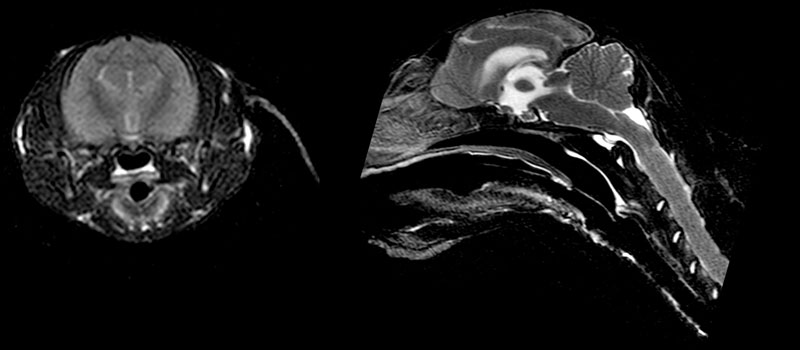
Incomplete fluid suppression with interstitial edema and/or ependymitis on transverse FLAIR MR image of a cat with FIP (corona virus). Sagittal T2-W shows generalized swelling and herniation.